
Update 22 Jan: Since posting this article yesterday, I have received some very persuasive comments echoing and expanding on my concerns. Please make sure you read the comments.
So, a few weeks into 2019, where do we think we are with M.E.? Are we making progress at last? Or are things very different from how they seem?
As far as I can tell, there has certainly been a positive feeling in the air ever since the helpful American IOM and P2P reports back in 2015 – and research in the U.S. does seem to be making progress these days, albeit with only a fraction of the funds which the NIH teasingly suggests should be coming our way.
Yet there is still a big question mark over things. Are we – and our wonderful biomedical researchers in the US – being hoodwinked? Are we being strung along and fooled into expecting funding that will never come? I don’t have the expertise to know for sure – but fortunately there are experienced bloggers such as Erica Verrillo and Jennie Spotila over there who can hold the authorities to account over this.
The modest grounds for optimism across the pond and in particular the NIH’s withdrawal of GET (graded exercise therapy) and CBT (cognitive behavioural therapy) as recommended therapies for our condition, coupled (possibly) with good old wishful thinking, have encouraged expectations in turn to be raised over here in the UK. The unexpected decision to review the NICE Guidelines for M.E. in spite of an earlier decision to leave them alone, coupled with reassuring noises about tearing them up and starting all over again, have been taken as further grounds for encouragement.
For many of us, however, all that hope dwindled away to nothing when the names were released of those who would sit on the NICE Guideline Review Committee, more than 50% of them transpiring to be adherents to the biopsychosocial theory of M.E. which has GET and CBT at its core. The possibility that GET and CBT would be withdrawn from the guidelines now seemed to many of us to be exceedingly unlikely.
Those in authority continue to say “trust us,” that all will come right in the end, and there are plenty who seem inclined to believe them. Yet it seems to me, even with only one eye on the Twitter feed – and sometimes not even as much as that – that in the UK at least, this time of waiting, poised on the edge of a better time which never quite seems to arrive, is going to come to an end. And not in a good way.
A lot of what is happening to make me reach this conclusion is going on ‘under the radar’. It is being talked about but only as ‘anecdotal evidence’, most commonly in the private corridors of Facebook groups, stories of those with various long term conditions, not just those like M.E. which the medics treat with suspicion, but all manner of highly respectable, fully accepted aches, pains and other unpleasant symptoms, controlled for years by repeat medications which are now slowly – and sometimes not so slowly – being withdrawn.
The excuse most often used for this is ‘patient welfare’. “The thing is,” the doctor explains to the patient who is sitting there shocked yet eager to please, though faced with the prospect of a lifetime of increased levels of pain or some other form of suffering , “patients are taking medication for one symptom which is then provoking a second symptom, which is then requiring a third medication to relieve it, and so it goes on. Through the side-effects, we are causing as many symptoms as we are treating.”
There is of course a great deal of truth in this, and doctors – and indeed patients – have known about it for years, yet the NHS has shown little intention to do anything about it, not until now. Now that the money is running out.
Occasionally, a little of what is happening makes the press. There has been widespread coverage, for instance, of the ban on prescribing numerous common drugs which are also available ‘over the counter’, sometimes at a lower cost than that of the prescription itself. This is arguably a sensible strategy for a cash-strapped NHS, though it is no laughing matter for those who until now have been entitled to free prescriptions but will now have to pay for these often essential drugs out of their own funds.
Less well publicised – and many would have thought more sinister – was a scheme in Oxfordshire reported by the Daily Telegraph to have been offering GP practices “cashback” for money they saved in cutting their expenditure on drugs prescribed to elderly patients in care homes. Practices were apparently told to ‘cut spending on medication by least £2 per care home resident”, then told they could ‘keep £1 per patient plus half of any more savings made’.
I’m pleased to say that local GPs were reported to have ‘lambasted the move’ but health officials apparently claimed that the incentives were to encourage doctors to ‘review the quality, safety and cost effectiveness of their prescribing’. So once again, the cost saving was being excused on the grounds of patient welfare. That report appeared in May 2017 and a Google search has revealed no further reference to such a scheme. Perhaps it has – quite rightly – been abandoned, but I can’t avoid the suspicion that it could equally well simply have been hushed up.
Reported more recently and more widely (in Feb 2018) were the ‘referral incentive schemes‘ run by CCGs across England, ‘offering GPs as much as 50% of any savings they can make’ by referring fewer patients to hospital. It would be interesting to take a look at some of the small print of that scheme. For instance, if a patient dies as a result of the decision not to refer, does the GP practice still get to keep the money? All CCGs were asked if they had such a scheme in place. Of the 180 that responded, 24% reported that they did.
Coming right up-to-date, there were widespread news reports just a few months ago of a new scheme in which rather than seeing the GP one to one, patients with long term health conditions would meet in groups of up to 15 at a time, spending much of this period ‘with a “facilitator” – a receptionist, clerk or healthcare assistant with a day’s training‘ (my underlining) – who can point them to advice on their health condition.
Hmm. This idea is also said to appear in the much vaunted Soviet-sounding NHS Ten Year Plan, which was in the news just the other day as I write, so they clearly still think it’s a great idea.
I suppose I admire the fact that for once they’re not actually claiming that seeing ‘a receptionist, clerk, or healthcare assistant with a day’s training’ is somehow safer than seeing a qualified doctor. I suppose we should be grateful they’re at last being honest about what they’re doing. The Daily Mail report states blatantly ‘the scheme is aimed at saving cash and doctors’ time’. At least we’re getting real here. Mind you, I doubt they’d dare to do that if these were ‘real’ i.e. life-threatening illnesses they were talking about. They are taking this step in the knowledge that they, the medical profession, and successive governments have spent a great deal of time and effort in convincing the population at large that long-term health conditions aren’t really diseases at all. They’re lifestyle choices selected by lazy people who just need someone with a day’s training to point out the bit of the screen they need to read and they’ll be right as rain again. And by ‘the population at large’, of course, we mean all the people who don’t have a long term condition. (Yet.)
Doctors will be on hand some of the time ‘to discuss tests and treatments’ with these fifteen people and you can see that this might free up some of their time by preventing unnecessary repetition. Even so, diseases vary from one to the other and from one patient to the next, and it seems to me that this idea might work better on paper than in practice.
Apparently ‘health chiefs say they want this approach to become the default care option for those with long-term conditions’, but they admit ‘the plans require ‘a leap of faith’. I can’t help but feel it is really the patients who are being expected to leap into the dark.
One potential benefit of this scheme that doesn’t get a great deal of attention in the coverage is the chance to discuss one’s condition with other patients. Whereas the group facilitator may have a single day’s training, some patients may have many years of experience twenty-four hours a day, at a level of understanding which only patients can share. Even if illnesses differ, patients may still have a lot to learn from each other. It seems to me that groups which understand and unlock this potential are likely to be the most effective, as opposed to those which focus on the day-long trained facilitator finding the right page to read out from her instruction leaflet.
The use of these crash-course trained facilitators ‘teaching’ a room full of patients in the internet age seems rather bizarre, and not surprisingly it reminds me of experienced patients at our local M.E./CFS clinic being taught – purportedly – how to manage their illness by someone who seemed to have just read the clinic leaflet for the first time the previous afternoon.
I doubt if this will be the only similarity between these new group sessions and CFS clinics. The publicity so far does not mention CBT, but this universal panacea is – according to the official figures – so cheap and so reliably effective, that it is difficult to imagine it not being added into the mix. In the new NHS, in which doctors are glimpsed across crowded rooms and drugs are withdrawn for health reasons, the all-effective CBT will surely be the saviour of the day.
I’ve written a lot here in recent times about ‘medically unexplained symptoms’ (MUS) and we’ve discussed the numerous other terms that are used with the same sort of meaning: psychosomatic symptoms, somatoform disorders, conversion disorders, idiopathic disorder, hypochondriasis etc etc… One word that is frequently used as part of these terms is ‘functional’, and I find it a particularly objectionable ingredient because it gives the impression of being the opposite of what it is. A ‘functional’ disorder gives the impression of being a systemic or mechanistic problem, something that clutters up the works and prevents the wheels going round properly. After months or perhaps even years of searching for what is wrong with them, patients often feel they’re finally making some progress when they’re told they have a functional disorder. They have no idea they’ve actually been told the opposite of what they think. They’ve been told that the doctor believes it’s all in the mind” after all.
Actually, if I’m going to be fair, most of the information online doesn’t actually say that any more. They’ve tightened it up in recent years, so it’s more likely to say something like “doesn’t appear to have a physical cause”. This may be a step in the right direction, but I’m not all that impressed. If they said something like “doesn’t have a physical cause which is currently understood but doctors will almost certainly find one in a few years time as medical science develops,” then I think that would be closer to the truth. Certainly, to judge by the attitude of most doctors to MUS/functional patients, “doesn’t appear to have” gets edited down to “doesn’t have” in their minds.
Anyway, the reason I have singled out “functional” from the morass of MUS terminology, is that the clinics for “functional neurological disorder (FND)” appear to be in the forefront of the MUS facilities we have been ‘promised’. The FND network is being expanded across the country.
These excerpts from the NHS A-Z website explain how the various acronyms (MUS, FND, and – perhaps not surprisingly – ME/CFS and CBT) fit together:

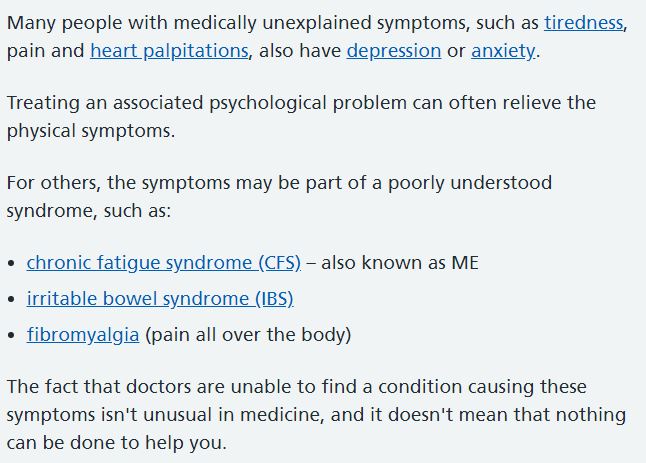
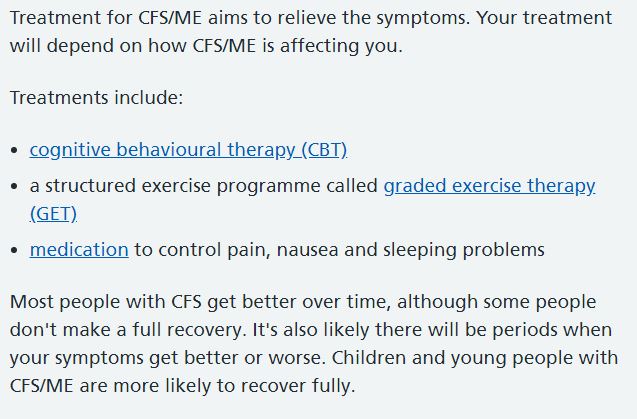
It’s strange how persistent misconceptions about M.E. can be, isn’t it? Unfortunately the majority of people with the condition do not necessarily get better over time though I have heard the theory time and again over many years. I was once given a massage by a lady who insisted that people usually recovered in six months and she couldn’t understand why I hadn’t. I expect she is still telling people the same thing all these years later. And of course CBT and GET are both recommended by this (presumably) authoritative NHS website, without any mention of the NICE guidelines being reconsidered. But what I am particularly wanting to highlight here is the purported link between CFS/ME and MUS. I suspect a similar link will be suggested between CFS/ME and FND.
According to the information on the net about the FND clinics, they seem to have some similarity with the ME/CFS clinics. A multi-disciplinary team typically provides CBT and GET or similar, for instance, but there is also often an emphasis on the presence of deep-seated trauma from past events, which is said to stem from an inability to express emotion. Most people with ME have been spared this far-fetched explanation for their symptoms but if they’ve been under the ‘care’ of, for instance, the Leeds inpatient clinic (aka The Yorkshire Centre for Psychological Medicine) they are unlikely to have escaped a weeks-long search for such a trauma.
I concluded an earlier post A Morass of MUS by suggesting that if in the future the NICE guidelines are indeed amended and the use of CBT and GET for ME is made more difficult by the growing weight of evidence against them, the diagnoses ME and CFS might be quietly dropped and new patients designated MUS instead, so that CBT, GET, and other psychological therapies could be used with freedom.
Could something similar happen with FND, I wonder? Having taken a brief look at the constituent parts of an FND clinic, all fitted out for CBT and GET – and now with the exciting added extra of treatment for deep-seated trauma – it seems likely that the authorities will consider these new facilities to be ideally suited for the treatment of what used to be ME/CFS. Why keep those ‘old’ unhelpful diagnoses if NICE makes them problematic? Why not say we have FND instead? We’ve long since asked to be treated as a neurological condition. Now it will suit them to give us what we want.
If you are not convinced that this is likely, look at this symptom picture:
People with FND often find they experience ‘sensory overload’ – lights feel too bright, noises too intrusive, heat and cold very uncomfortable, uncomfortable skin sensations (tingling, crawling, prickling, tenderness or pain). The difficulty with ‘gating’ may also cause problems with concentration.
A common FND sensory symptom is pain. The pain is often but not always difficult to locate and seems to come from muscles, skin or joints at various times. It gets better and worse, and is usually combined with a feeling of intense tiredness or fatigue, and difficulty concentrating…
When someone is struggling to concentrate, they are not able to filter out unimportant sensory information to focus on what is important. People who are trying hard to overcome their difficulty concentrating or problems filtering sensory information often feel exhausted or fatigued a lot of the time. These symptoms are very common with FND.
A person with FND may often complain of memory problems. This is often a result of finding it difficult to concentrate. As a result you might lose things, such as keys, or find you have put the kettle in the ‘fridge’ instead of back on the worktop. You may forget appointments or things that you have done recently, and often feel that your brain is in a ‘fog’. You might also feel extremely fatigued.
The fatigue usually varies day to day, but characteristically if you overdo it one day you pay for it the next and have to take more rest to compensate. Some people complain that the fatigue is so intense, for example, that they have to spend a day in bed after they have been shopping, yet on other days they feel very bright.
The above is an extract from a description of FND symptoms taken from the Sheffield FND clinic website. ‘Gating’ is a term which relates to difficulty in filtering sensory information and is used as the explanation for many FND symptoms including heightened sensitivity to light, noise, temperature etc which we know in the case of M.E. to be caused by hypothalamic dysfunction. Setting this difference to one side, however, the above could be a description of a great many symptoms of M.E. Bearing this in mind, I don’t find it too hard to imagine people with M.E. in the future – newcomers perhaps not even aware of ME/CFS – being treated in a clinic for FND, deep-seated traumas and all. As ME/CFS would no longer be the diagnosis, the ME/CFS Guidelines could be ignored.
So how does this affect our present concern with NICE?
I am starting to wonder if the late decision to revise the guidelines was really a strategic ploy in a much larger game: a ploy to keep us all focused on a detail which would soon become irrelevant. A ploy to keep us looking out of the train window, squinting at the appointments to the Guideline Development Group, trying to guess if there’s still a chance that CBT and GET will be removed in a couple of years, all the time unaware of what is heading towards us down the line ahead, a monstrous train which is bent on headlong collision.
And what exactly is this nightmare train?
The future of British medicine, the future of the NHS, a future which no longer has the funds to deal with chronic illness and so prefers to pretend it doesn’t exist. A future in which ‘unhelpful’ medicines used for years are taken away, patients meet with each other instead of with doctors, and people with symptoms that are not understood are – more than ever before – assumed to be mentally ill.
A future in which a large proportion of what we used to know as medicine has been subsumed by psychiatry.
Meanwhile those with genuine mental health problems can’t get the treatment they need because those who should be helping them are treating the physically ill. I must admit that I can’t work that one out. Why are the psychs so keen on treating the physically ill when they can’t provide enough care for those with real mental health issues? Could it be that they simply find those who are genuinely mentally ill too demanding and prefer to treat us instead?
And what about the once mighty drug companies? How do they feel about all those drugs being taken away? I can’t work that one out either. I assume they must have a plan but I doubt that it helps the rest of us.
But these details aside, I’m afraid the rest of the picture seems to make perfect sense. It’s all about saving money, and we will all suffer because of it.
It’s ironic. All this time, we patients with M.E. and other ‘misunderstood’ conditions have wanted to be treated the same as other people with chronic illness. Now it’s going to happen, but not in the way we had hoped.
Things aren’t going to get any better for us. They’re going to get worse for us all.
*************************************************************************************
After all the above, it’s rather ironic that – as I mentioned last time – I have recently published a creepy (and funny) children’s fantasy story. This explains the incongruous ad you may have glimpsed in the sidebar. Please be kind to me and take a look at all the excellent reasons why you should get yourself a copy. And no, Grimly Darkwood isn’t my real name any more than Spoonseeker is.
Anyway, let’s hope the post you’ve just read turns out to be a fantasy story too. I really hope it does. With all the posts I’ve done on MUS, I’ve been scared of unnecessary scare-mongering and I’ve thought long and hard before publishing, but I think it’s important that we all express our concerns. These are strange times we live in and it’s not always easy to know what will happen next.

“And what exactly is this nightmare train?”
Well, you’re on the right track, it’s MUS, and IAPT, and LTC. All together the plan is to decimate our secondary care services by convincing doctors that patients have mental health conditions that must be prioritized over physical healthcare with cheap online treatments and computer apps.
And in relation to ME/CFS? It’s to use the IAPT MUS data set in the NICE Guidelines review as evidence for the effectiveness of CBT and GET for ME/CFS patients, patients who of course haven’t been properly diagnosed using a robust definition such as ICC, but rather have been persuaded to attend by their doctors who don’t know what else to do with them, and who are then given the Chalder Fatigue questionnaire. It’ll all become clear if you read this paper –
Barkham, M., Moller, N. P. and Pybis, J. (2017), How should we evaluate research on counselling and the treatment of depression? A case study on how the National Institute for Health and Care Excellence’s draft 2018 guideline for depression considered what counts as best evidence. Couns. Psychother. Res., 17: 253–268. doi:10.1002/capr.12141
and then contemplate the purpose of Dr Phil Hammond’s slot in the upcoming NICE Conference – that’s what is meant by ‘real data’.
LikeLiked by 1 person
Thank you – I will take a look at that reference.
LikeLike
For those who are not aware, Sir Simon Wessely will be talking to Dr Phil Hammond at the NICE conference about ‘how the NHS can make integrating physical and mental healthcare a reality.’
LikeLike
Yes, but I was referring to the other Phil Hammond slot – “Reliable evidence?: The roles of real-world data, patient evidence and randomised trials in judging treatment effectiveness” where Phil Hammond is the chair. – http://www.niceconference.org.uk/agenda . Sorry, I should have made that clear.
LikeLiked by 1 person
Right, Couch Turnip, I have been through the paper you mention (Barkham et al) using my own unique form of speed reading which involves zoning out during all the difficult bits, so perhaps you can tell me if I am on the right lines?
This appears to be a policy document masquerading as a piece of research. At a stroke, it overturns the long accepted superiority of quantitative over qualitative research, arguing that the latter allows the patient voice to be heard, and paves the way for greater diversity of research evidence, so allowing greater diversity of available treatments. In other words, it allows NICE to specify whatever treatments they like irrespective of what used to be called ‘the evidence’.
In downplaying the importance of qualitative research, it removes one of the planks of argument against the PACE trial but this is scarcely important as the whole idea of this strategy is to render this discredited trial irrelevant.
The paper paves the way for the use of low quality data sets such as the IAPT MUS data which can then be used to justify the use of GET and CBT for ME/CFS without reliance on PACE.
Do I have the gist of it?
LikeLiked by 1 person
That’s just about how I interpreted it. They appear to say that consideration of the the IAPT dataset in the NICE guideline review for depression would be consistent with the NICE guidelines manual. Presumably the same would apply to the ME/CFS NICE guidelines review. If there’s a lessening of the superiority of the randomized trial/RCT in the NICE evidence stakes then that would mean a lessening of the importance of the heavily criticized PACE Trial. It would be interesting to know what’s said at the NICE Conference.
LikeLiked by 2 people
In the US we have been co-opted by a successful public relations campaign. NIH Director “Lucy” Collins keeps promising to help us Charlie Browns, and we seem to mostly believe that *this* time he won’t pull back the football and leave us flat on our backs. But he always does, and always will.
The real question is, exactly who is controlling the Policy of No Research? The answer, of course, is “follow the money” but apparently no one wants to go there…
LikeLiked by 2 people
I’m afraid your Charlie Brown metaphor rings very true – and I fear that something much the same is happening over here. Thanks for your comment.
LikeLiked by 1 person
It always pays to follow the money. In the UK the London School of Economics LSE is at the centre, working in conjunction with the Institute of Psychiatry, Psychology and Neuroscience (IoPPN) [or Institute of Psychiatry IoP as it used to be called] to reduce the healthcare budget by tens of billions of pounds. The Government insists that they want ‘parity of esteem for mental health’….. what a joke. What they actually want is to keep patients out of physical healthcare services by claiming that they are mentally ill. This is hidden behind the façade of ‘integrating mental and physical healthcare’. It’s working rather well and very sick patients are being turned away and denied any care.
LikeLiked by 3 people
You clearly have access to more information than me, and you put it more clearly than I could. But the intended message is the same. It needs to be shouted from the rooftops. I will tweet tomorrow and link to these three letters, this last one in particular. The message could not be more simple – or more chilling. Thanks for sharing it. Thanks also to jimells.
LikeLike
LSE ‘at the centre’ is interesting. Are you able to share how you know about that?
LikeLike
Martin Knapp at the LSE (also IoP) has been behind making the economic case for IAPT MUS and many other money saving health interventions. Note his 2012 article – ‘Mental Health in an Age of Austerity’ where he makes the case that addressing people’s mental health problems can save the NHS money. There are many reports but this influential report – HOW MENTAL ILLNESS LOSES OUT IN THE NHS
a report by The Centre for Economic Performance’s (CEP) Mental Health Policy Group – was compiled by a group including – Martin Knapp (LSE and IoP), IAPT co-founders Lord Layard (LSE, CEP) and David Clark (Ex-IoP, Oxford Uni), Michael Parsonage (Centre for Mental Health) and Simon Wessely (IoP) amongst others.
LikeLiked by 1 person
I should have added to my first comment – NHS Digital is a stakeholder in the ME/CFS NICE guidelines review. They collect all the IAPT data. One has to wonder that if patients in the IAPT MUS arm aren’t improving, could they be redefined as anxiety or depression patients instead so that the MUS outcome measures aren’t reported?
Alternatively, if the final questionnaire isn’t filled in, or if one of the Chalder Fatigue Questionnaires is somehow lost, then the client would be moved out of MUS as I understand it and just their anxiety and depression scores would be entered into the data collection. I don’t know that this is happening to any extent, but it’s a way that the figures could potentially be fixed to provide evidence that CBT and GET are effective. And we know that IAPT is incentivized and that some services are operated by private companies.
LikeLiked by 3 people
Interesting reads that I’m only just catching up on. (y)
One thing that struck me, on reading your quotes of the FND symptoms picture, is that ‘Jon’ actually just copied it straight from M.E. diagnostic criteria in order to save time and effort, and be sure to catch everyone with M.E. in his expanding FND net. It’s far to close to an M.E. description to be a coincidence.
LikeLike